Day 71 – May 26, 2020
There’s an interesting footnote about that Spanish Flu pandemic of 1918… which is the age distribution of deaths. For COVID-19, the median age of mortality is… well, it’s high. Depending where you look, it’s almost always north of 80. The younger you are, the better your chances… all the way down to zero, where except in extremely rare cases, often associated with other contributing factors, pretty-much anyone under the age of 20 looks safe from developing any serious symptoms.
A lesser-discussed pandemic is the Russian flu, which ran over a period of 4 years, peaking around 1890… and ultimately killing more than a million people worldwide. Its mortality profile is similar to COVID-19 in that it was far more dangerous for the elderly. But also, a big difference… is that it also killed a lot of very young people. The mortality rate for ages 0 to 10 was similar to those somewhere in the 40-60 range. The 10-30 age range was the least affected… and those over 70 were more than 20x likelier to die than that 10-30 group.
The 1918 pandemic hit the young people the hardest, a puzzling question that’s still being discussed, and there are very different ways of approaching it. The worst age to be for that pandemic was 28 — that was the highest-mortality age group. One common thought is that those who survived the 1890 pandemic built immunity, and were far less affected in 1918. But another interesting analysis starts with some simple math… 1918-28 = 1890. Indeed, those who survived the 1890 pandemic as infants… whether just born or perhaps still in utero — they were the ones hardest hit 28 years later.
To further confuse the issue, while it’s established that 1918 was without a doubt influenza (H1N1), there are some theories that 1890 wasn’t actually a flu, but a coronavirus… which obviously means that the theory of acquired immunity for older people can’t be correct, and that perhaps some drastic effect on the immune system of infants took place during a critical time of development.
Such are the sorts of things I learn when I fall into the Google spiral of doom… setting out to research something, and winding up very far away… and you all know how that can go… even here on Facebook, you log in to just send a quick message to a friend, and 20 minutes later you’re looking at wedding pictures of people you’ve never heard of.
What I started with today has to do with headlines like this:
“Coronavirus cluster linked to pool party” (Arkansas)
“Several members of a Franklin church test positive for COVID-19” (North Carolina)
“A second hairstylist potentially exposed 56 clients to COVID-19” (Missouri)
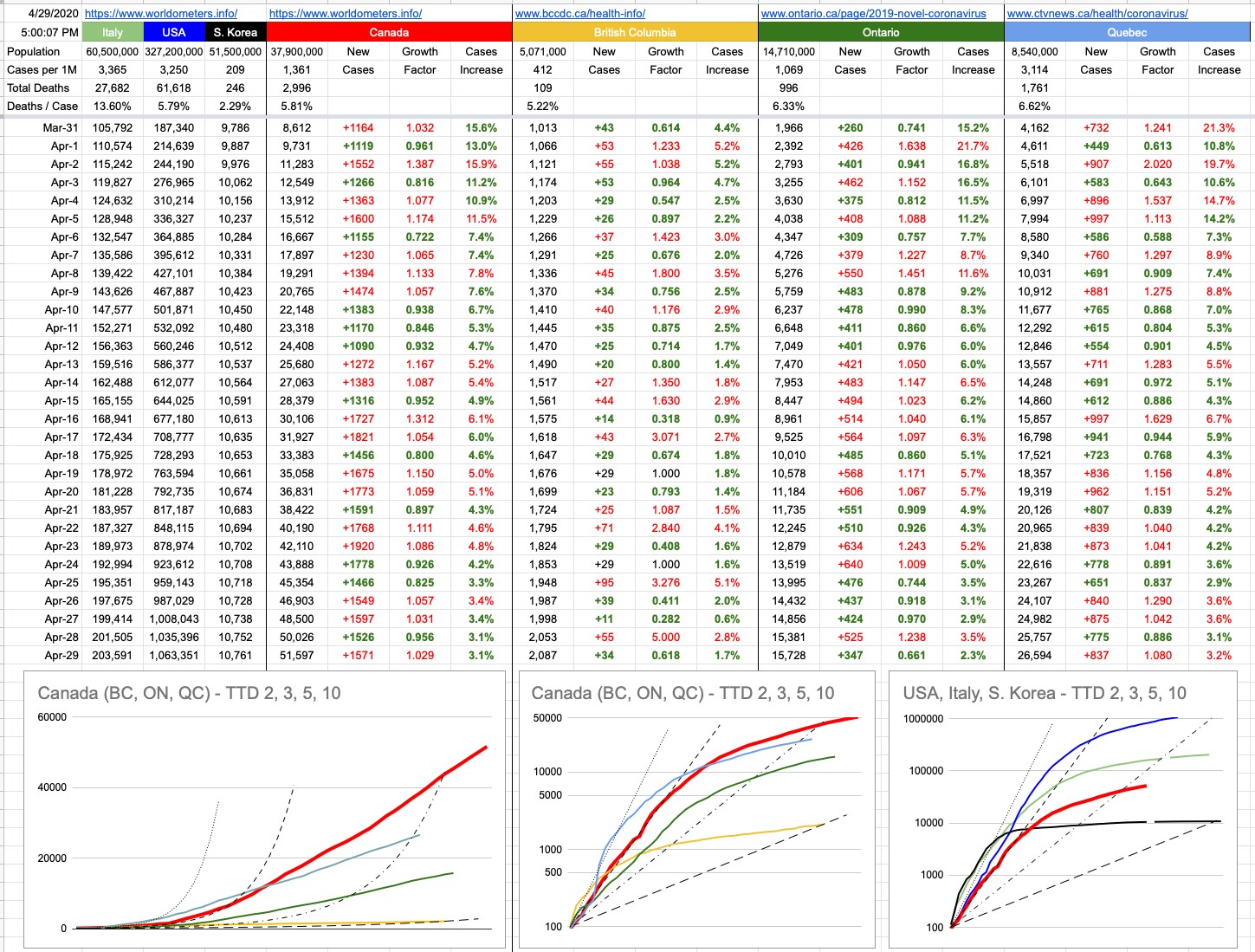
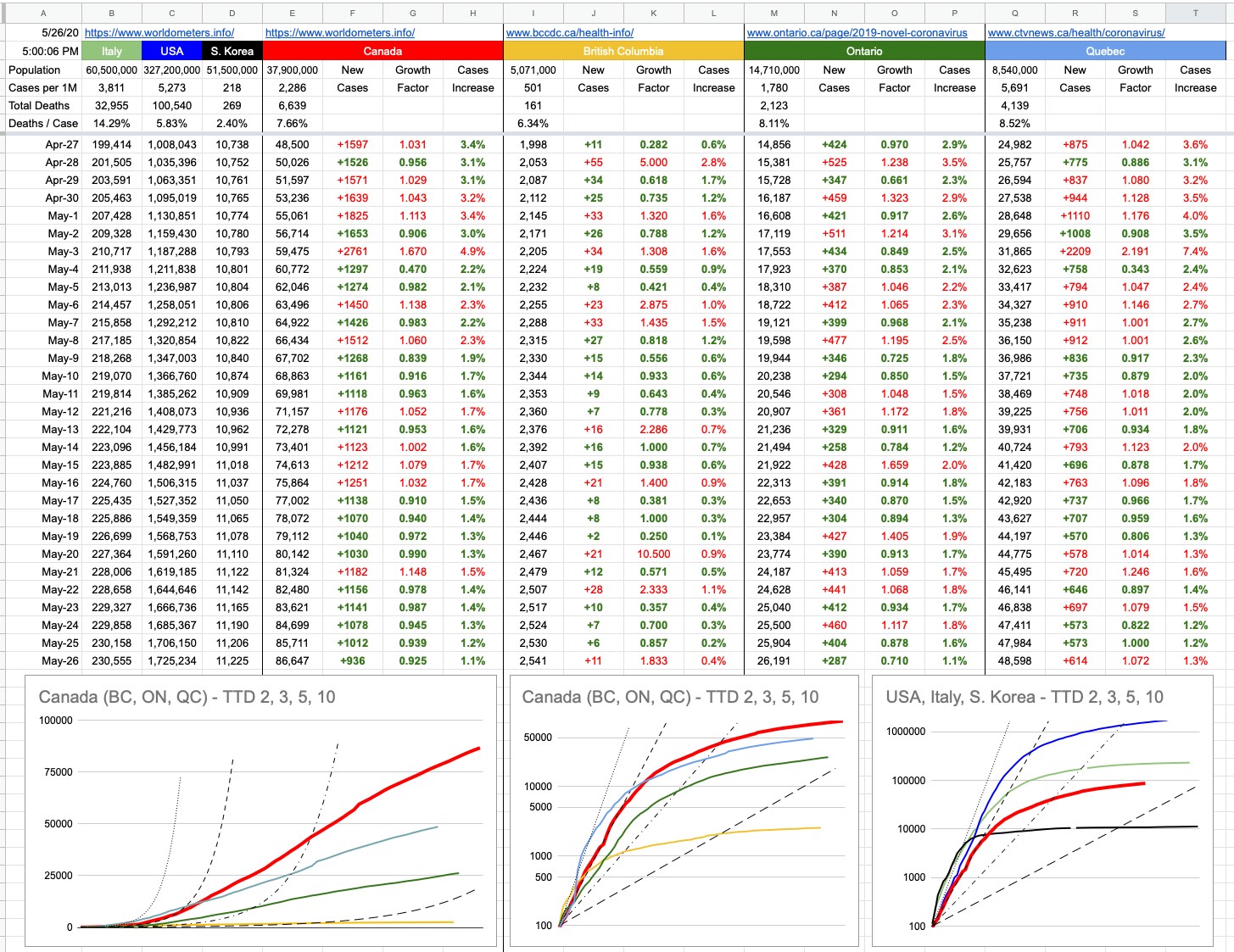
When I started writing this today, the American death count was below 100,000. As I prepare to hit [Post], it’s now over…
Some American states violently threw the doors open at the start of May — so now we’re seeing not just the initial effects, but the secondary ones as well. With an incubation period of 5 to 14 days, we’re perhaps even seeing the beginnings of a third. So how does it look… well, in 17 states, the numbers of new cases are trending upwards… among them Arkansas, North Carolina & Missouri. And Georgia. And Alabama. It’s really not a big surprise to see where things aren’t headed in the right direction. And there’s no reason to single out the U.S. — we’ve all seen those pictures from that park in Toronto a few days ago. I went for a great bike ride today, and my usual ride would have taken me down the Arbutus corridor, down to the water, and around the seawall… with a lap of Stanley Park if time (and regulations) permit. But I avoided all that, because I didn’t want to be anywhere near the sort of crowd I imagined I’d find.
The vast majority of people whose behaviour really makes you wonder… are younger. Because, you know, they’re invincible. And I don’t mean to single out an entire generation or two as irresponsible; it’s just what I happen to observe around me.
And when you think about it, I’m double their age and even I can’t really say I’ve suffered through any global health crisis that’s affected me. I’m old enough that certain vaccines didn’t exist when I was a kid, so I, along with most of my peers, suffered through chicken pox. The MMR vaccine showed up a few years after I was born, which means I missed the ideal window to have gotten vaccinated. I did, of course, as soon as it made sense… but anyone younger than me… they’ve largely been immune from birth… to diseases which, not that long ago, would’ve been affecting — and possibly claiming the lives of — friends all around them.
“The risks are for the history books and life is meant to be lived and we’re not really at risk, etc etc.”
It’s not a great attitude, in general… and it applies to everyone who thinks for some reason we’ve made it free and clear to the other side. We haven’t, yet. Opening up doesn’t mean throwing caution into the wind.
View Original Post and All Comments on Facebook